Image Challenge
To promote critical thinking as well as friendly rivalry, the image challenge was implemented. By distributing images with a clinical vignette, residents and faculty test their medical knowledge by answering questions of diagnoses and management.

Challenge 1
young gentleman who received several abrasions 2 months ago while swimming in Brazil on his honeymoon. His other abrasions all slowly healed but this one on his abdomen slowly enlarged and is now very tender (initially painless). He received Keflex and did not get better - he thinks the lesion is still actually getting larger. What is the diagnosis?
Flip panel for explaination
Diagnosis: Leishmaniasis
What we learn: Transmitted via bite from the female sandfly and of the new cases, 90% of cutaneous leishmaniasis happen in the following nations:
(1) South America – Brazil and Peru
(2) Middle East/Africa – Afghanistan, Pakistan, Syria, Saudia Arabia, Algeria
The skin forms are the most common and can range from nodules to gross mucosal tissue destruction. Diagnosis is by skin biopsy and that will sometimes show intracellular organisms; however if you have the clinical suspicion, biopsy samples can also be sent to CDC for PCR and DNA sequencing. There is limited data about the treatment options available but can include pentamidine, amphotericin B, and miltefosine. This gentleman received liposomal amphotericin B because of the size of his lesion. Many of us were thrown by the history he was swimming in Brazil - a red herring!

Challenge 2
This is a 53 yo M who is presenting with a 15 month history of worsening difficulty with chewing foods, dysphagia as well as changes in his speech. On examination of his tongue, you note the above. Diagnosis?
Flip panel for explaination
Diagnosis: ALS (Amyotrophic Lateral Sclerosis) with bulbar symptoms
The tongue findings above represent tongue atrophy and his symptoms involving changes in his speech and dysphagia are classic bulbar symptoms.
ALS, also known as Lou Gehrig’s Disease is a progressive neurologic disorder characterized by degeneration of both the upper motor and lower motor neurons. Unfortunately, there is no cure for the disease and death by respiratory paralysis occurs within a span of typically 3-5 years.
Most commonly, symptoms first begin with the limbs but up to 1/3 of cases can present with bulbar symptoms. Other physical exam findings may include muscle fibrillations as well as decrease strength in a mixed upper motor neuron (spastic tone, hyperreflexia) and lower motor neuron (flaccid tone, hyporreflexia) pattern. Typically, eye findings and loss of bowel/bladder control are late findings.
No single test will provide a definitive diagnosis. Rather, the diagnosis is made with history, physical exam findings in conjunction with EMG, MRI and laboratory studies ruling out other potential causes.
Challenge 3
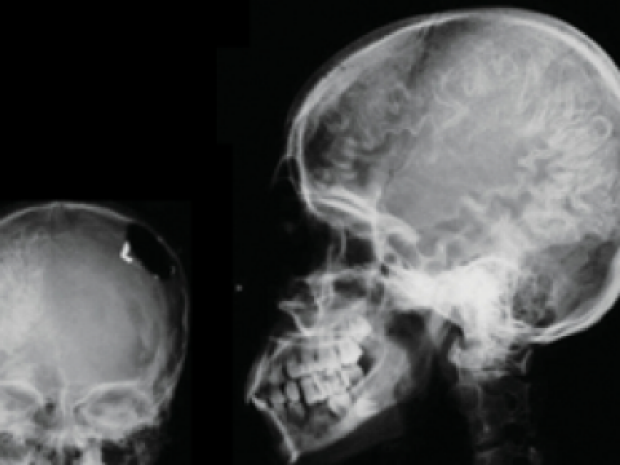
A young female comes into clinic after a fall with focal pain over the right temporal region and has skull radiographs done. She has a history of seizures ever since early age and is maintained on phenytoin.
What is the finding on the skull radiograph (1 point) and what is her underlying diagnosis (1 point)?
Flip panel for explaination
Diagnosis? Sturge-Weber angiomatosis. This is a rare congenital (not hereditary) condition with facial capillary malformation (port wine stain) and capillary-venous malformations in the brain and eye. Because of the effect of these malformations in the brain, patients usually have seizures and developmental delay.
Port-wine stain: capillary malformation seen in Sturge-Weber. However, just because a child has a port-wine stain, does not mean they have Sturge-Weber.

Finding on Skull Radiograph? Tramline calficiations – these happen because of angiomas affecting the leptomeninges. The intracerebral capillary-venous malformation usually occurs on the same side as the port-wine stain.

Challenge 4
A young woman presents to the ED with diffuse pruritus as well as the lesions you note above. She has a history of SLE and is taking systemic steroids. On physical exam, you note the lesions bilaterally on her hands, elbows, feet, and scalp. What is the diagnosis (1pt) and what oral agent would you give her for treatment? (1 pt)
Flip panel for explaination
The answer is crusted (or Norwegian) scabies. This is a rare but very severe form of scabies that often occur in immunosuppressed patients (ie AIDS, patients on high doses of immunosuppressives) but can also occur in patients who have sensory/motor neuropathies as well as in demented patients. This disease is HIGHLY contagious given the high mite burden. While scabies in its normal/mild form in typically treated with permethrin cream, crusted scabies will also require use of oral ivermectin in addition to permethrin topically.
Challenge 5
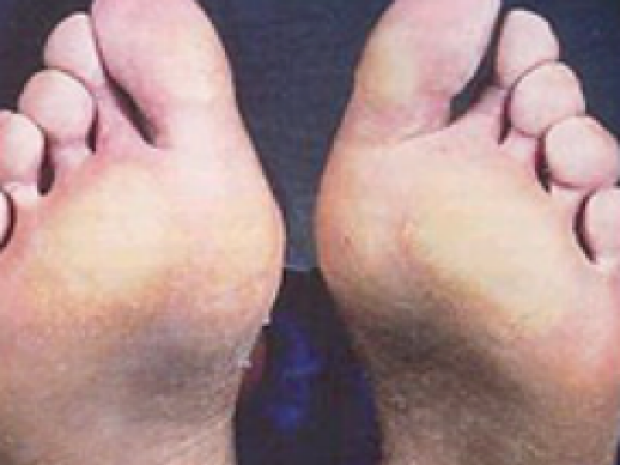
A 32 y/o M comes into your primary care clinic for evaluation of 5 months of progressive dysphagia with the sensation of food sticking in mid chest and the above findings. You notice he has similar changes on the palms of his hands.
What are the findings on hands and feet (1 point) and what is the unifying diagnosis (1 point)?
Hint: this is not CREST syndrome.
Flip panel for explaination
Skin Findings? This patient has palmoplantar keratoderma, which is thickening of the skin over the palms and soles.
Diagnosis? This gentleman has Howel Evans Syndrome, which refers to an autosomal dominant form of palmoplantar keratoderma that is associated with wax-like hyperkeratosis of the palms and soles and a substantially increased risk for esophageal squamous cell carcinoma. This is also known as tylosis with esophageal cancer. Sometimes these patients also have oral leukoplakia.
The American Society of GI Endoscopy recommends endoscopic surveillance for esophageal SCC starting at the age of 30 y/o and recommends surveillance at least every 1-3 years.*
Challenge 6
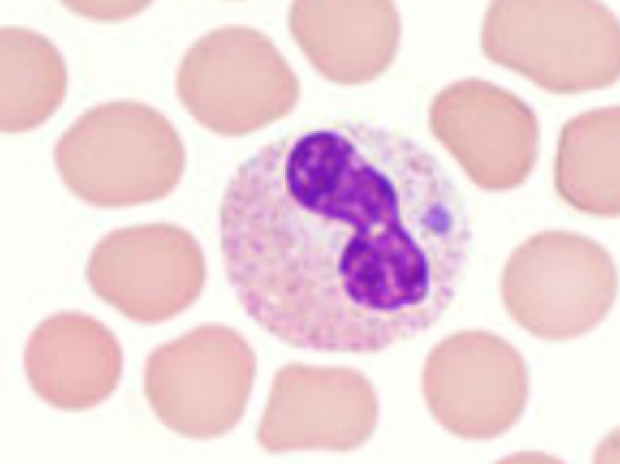
A 58 year old man recently returns from visiting relatives in Minnesota approximately 10 days ago. He is presenting with headache, fevers, and myalgias. On blood smear, you note the above. What’s the diagnosis?
Flip panel for explaination
Solution: Human granulocytic anaplasmosis. Credit was given for ehrlichiosis as well given difficulty distinguishing it from anaplasmosis based on clinical information. However, it should be noted that human granulocytic anaplasmosis typically infect granulocytes (eosinophils, basophils and PMNs) whereas ehrlichiosis infect monocytes.
Further discussion:
Anaplasmosis (caused by the bacteria Anaplasma phagocytophilum) and ehrlichiosis (caused by the bacteria Ehrlichia chaffeensis) are a group of tick-borne (Lone star tick) obligate intracellular bacteria found mostly in the midwestern and northeastern regions of the US. The incubation period is typically 1-2 weeks. Presenting symptoms are often nonspecific and include fevers, headaches, malaise and myalgias. Laboratory findings include leukopenia, anemia, thrombocytopenia, and elevated LFTs. On blood smear, a morula, or a intracytoplasmic inclusion (seen in our patient) is often a very specific, though not sensitive marker of infection. Serologic studies can be used for confirmation, looking for a four fold change in antibody titers between acute and convalescent phases of the illnesses. PCR can also be used but sensitivity often drops after the acute phase. Treatment is typically with doxycycline and should not be delayed while awaiting confirmatory diagnosis if suspicion is high.
Challenge 7
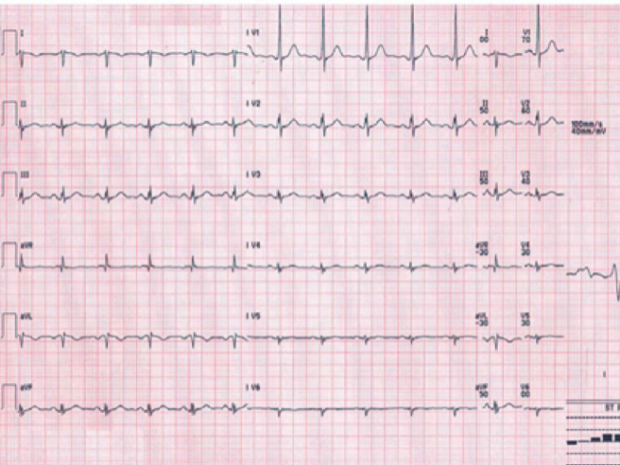
A 43 y/o gentleman with history of sinus infections presents to your clinic with recurrent cough with the EKG shown above. Diagnosis?
Flip panel for explaination
EKG demonstrates dextrocardia with tall R waves in lead V1 and absent R wave in V6. Lead misplacement can also cause this appearance of EKG. To confirm if dextrocardia vs lead misplacement, confirm lead placement and can obtain R sided chest leads (in dextrocardia will demonstrate normal progression of R wave amplitude).
Diagnosis is Kartagener's Syndrome which is an autosomal recessive disorder in the function of cilia and is classified under group of disorders called Primary Ciliary Dyskinesias. The classic triad for Kartagener's Syndrome:
(1) Chronic sinusitis
(2) Bronchiectasis
(3) Situs inversus
These patients generally present with recurrent upper and lower respiratory tract infections because of ineffective mucocilliary clearance. Males are generally infertile because sperm motility is dependent on ciliary function.
Roughly 50% of patients with primary ciliary dyskinesias have situs inversus totalis - complete reversal of the circulatory system and viscera. This is thought to occur because in early embryonic life normal ciliary function is necessary to develop normal laterality, which is disrupted in Kartagener Syndrome.

Challenge 8
This is a 58 year old gentleman who was reminded by his wife to ask you about the skin findings above on his back, which she has noticed in the recent two months. On further questioning, he states that he has had some vague symptoms of fatigue and decreased appetite over the past few months but has otherwise felt at his baseline. What is the skin finding (one point) and what is the most likely underlying diagnosis (one point)?
Flip panel for explaination
EKG demonstrates dextrocardia with tall R waves in lead V1 and absent R wave in V6. Lead misplacement can also cause this appearance of EKG. To confirm if dextrocardia vs lead misplacement, confirm lead placement and can obtain R sided chest leads (in dextrocardia will demonstrate normal progression of R wave amplitude).
Diagnosis is Kartagener's Syndrome which is an autosomal recessive disorder in the function of cilia and is classified under group of disorders called Primary Ciliary Dyskinesias. The classic triad for Kartagener's Syndrome:
(1) Chronic sinusitis
(2) Bronchiectasis
(3) Situs inversus
These patients generally present with recurrent upper and lower respiratory tract infections because of ineffective mucocilliary clearance. Males are generally infertile because sperm motility is dependent on ciliary function.
Roughly 50% of patients with primary ciliary dyskinesias have situs inversus totalis - complete reversal of the circulatory system and viscera. This is thought to occur because in early embryonic life normal ciliary function is necessary to develop normal laterality, which is disrupted in Kartagener Syndrome.

December 2017, Challenge 8
A young adult gentleman with no past medical history presents to clinic with 1 week of bleeding gums. He has had 3 weeks of fatigue and decreased appetite with an unintentional 12-pound weight loss. Examination is notable for tender cervical and submandibular lymph nodes as well as the gums seen in the image.
Flip panel for explaination
Explanation:
His CBC was notable for WBC of 194K with 40% blasts and platelets of 12,000/mL. Bone marrow biopsy showed acute myelomonocytic leukemiaand he was diagnosed with leukemic gingival infiltration.
Leukemic infiltration of the gingivae has been associated with monocytic variants of AML (M4 and M5 subtypes). There are several case reports of AML in the literature presenting as gingival hyperplasia, bleeding, and/or pain. In these case reports, after appropriate treatment of the AML, the gingival pathology improves.
Challenge 10
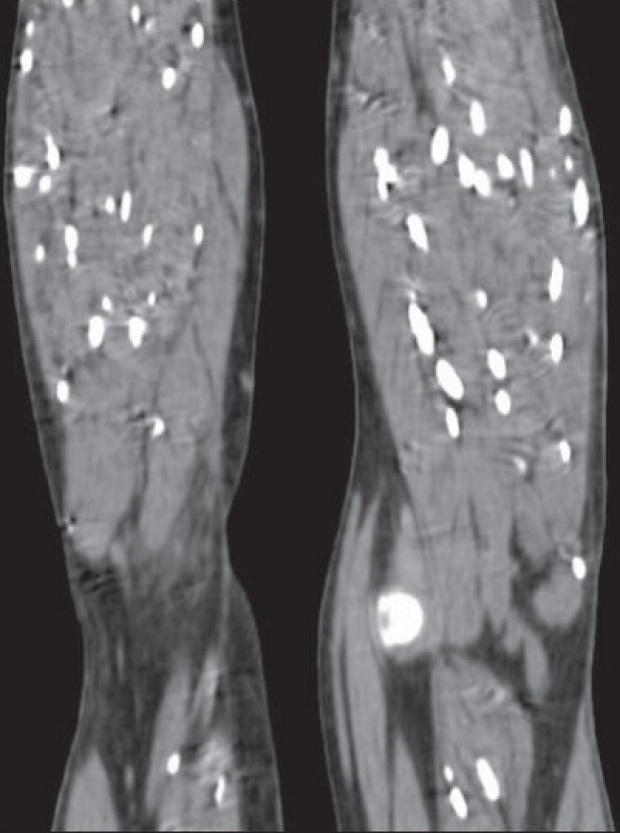
A 43 yo gentleman who recently moved from India is presenting with several month history of worsening bilateral leg pain. During this time period, he has also noted development of headaches. On physical exam, you note hypertrophy of the leg muscles. A MRI of the legs was obtained demonstrating the following:
Flip panel for explaination
Solution: Disseminated cysticercosis. Patient likely had both neurocysticercosis based on his headaches as well as extraneural cysticercosis based on his MRI findings of the calcified cysts.
Cysticercosis is a parasitic illness that develops after a person ingests Taenia solium (pig tapeworm) eggs through fecal-oral transmission. Because humans are not the natural host, the larvae bury themselves into human tissue instead of developing into tapeworms. Depending on where the cysts are found, the disease is either labeled as neurocysticerocis or extraneural neurocysticercosis. The disease endemic to Central and South America, Sub-Saharan Africa, India and other parts of Asia.
The incubation period is typically 3-8 weeks. While most people are initially asymptomatic, the cysts eventually lose their ability to affect their host's immune system, leading to increased inflammation, causing symptoms such as edema, seizures, strokes, pain, and cardiac conduction abnormalities if found in the heart.
Diagnosis is often made based on history, exam, and radiographic studies. Serological testing is sometimes helpful as well, particularly when imaging studies are nondiagnostic. Rarely, biopsy is required.
Treatment for disseminated cysticercosis often includes a combination of antiparasitics (most often albendazole and praziquental) in addition to steroids. Antiepileptic drugs are used in adjunct for patients who present with seizures. For patients with isolated intramuscular cysticercosis, symptomatic management with NSAIDs and excision alone can be considered.

Challenge 11
A 36-year-old gentleman with history of heavy alcohol abuse presents to the emergency department with severe abdominal pain. You note the findings noted on the image when examining his abdomen. What is the name of this sign (1 point) and what is the underlying diagnosis (1 point)?
Flip panel for explaination
This is periumbilical ecchymosis and is called Cullen’s Sign. This was first described in a case of ruptured ectopic pregnancy (as Kelly shared with all of us!), but can be seen in any case of intraabdominal hemorrhage. In this patient, who has heavy alcohol use, the finding suggests acute pancreatitis. In pancreatitis, Cullen’s Sign occurs from pancreatic enzymes causing fat necrosis and inflammation with resultant intra-abdominal bleeding and is therefore seen in severe necrotizing pancreatitis.

Challenge 12
A 64 year old man with a history of latent TB s/p treatment as well as mitral valve prolapse presents with progressive worsening dyspnea over the past two days. He notes occasional cough productive of pink tinged sputum but otherwise denies fevers or chills. CBC, BMP, and procalcitonin are within normal limits. What is the underlying cause of the CXR finding?
Flip panel for explaination
Solution: Unilateral pulmonary edema caused by mitral regurgitation.
Discussion: Unilateral pulmonary edema accounts for about 2% of all cases of pulmonary edema and it is most commonly associated with mitral regurgitation. It is hypothesized that the eccentric regurgitant jet is predominantly directed at the right superior pulmonary vein and thus causes increased hydrostatic pressure in the R upper lobe, causing asymmetric pulmonary edema. Other less common causes of unilateral pulmonary edema include positioning, re-expansion pulmonary edema, pulmonary vein occlusion, R to L shunts and hypoplasia of the pulmonary artery.
Challenge 13
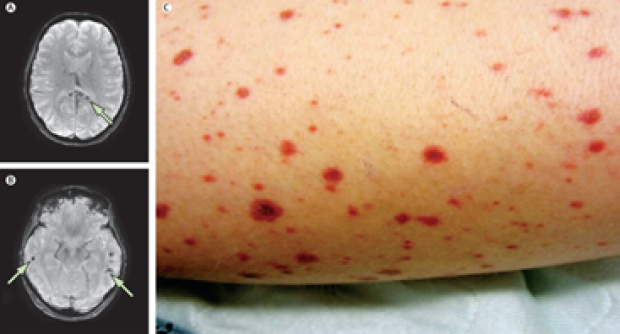
A 28-year-old woman with history of HIV presents to the hospital via ambulance for 5 days of fevers and disseminated rash (pictured above on her leg) and 1 seizure episode that occurred on the day of presentation. She underwent MRI during her admission with images shown.
Flip panel for explaination
Solution: She was diagnosed with Zoster-associated encephalitis from disseminated VZV. Zoster-associated encephalitis usually develops within days of the disseminated rash, as was seen in this patient, and should be an important consideration when immunocompromised patients present with acute delirium or neurologic symptoms. Patients can present with symptoms of an acute stroke depending on the distribution of the VZV vasculitis. When this is suspected, patients should be started on IV acyclovir.
Challenge 13
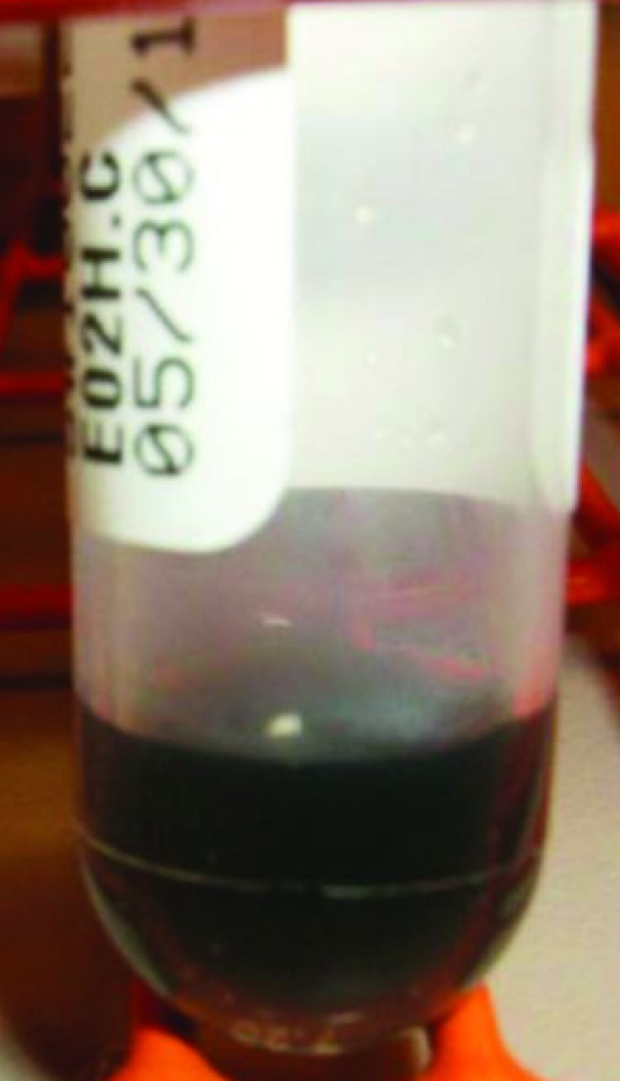
A 34 yo woman presents with malaise and fatigue. Her serum sample is shown here. What is the underlying diagnosis?
Flip panel for explaination
Solution: methemoglobinemia
Further discussion:
Methemoglobin is an altered form of hemoglobin in which the ferrous (Fe++) iron of heme are oxidized to the ferric (Fe+++) state, giving the serum the classic blue-brown appearance. Methemoglobin irreversibly binds oxygen, unlike hemoglobin and thus shifting the oxygen dissociation curve to the left. Symptoms are nonspecific and include lethargy, headaches, fatigue and dyspnea. The diagnosis should be strongly suspected in hypoxia without response to oxygen supplementation as well as cyanosis in the setting of a normal PaO2.
Two forms of methemoglobinemia exists: congenital and acquired. In the congenital form, there is reduced enzygmatic conversion of methemoglobin to hemoglobin. Usually patients present with cyanosis but otherwise are asymptomatic. In the acquired form, drugs or other compounds cause an increase in methemoglobin in the body. Common drugs that cause methemoglobin include dapsone and topical anesthetics (lidocaine, benzocaine, etc).
Treatment of methemoglobinemia typically involve methylene blue and ascorbic acid.